



 로그인을 해주세요
로그인을 해주세요
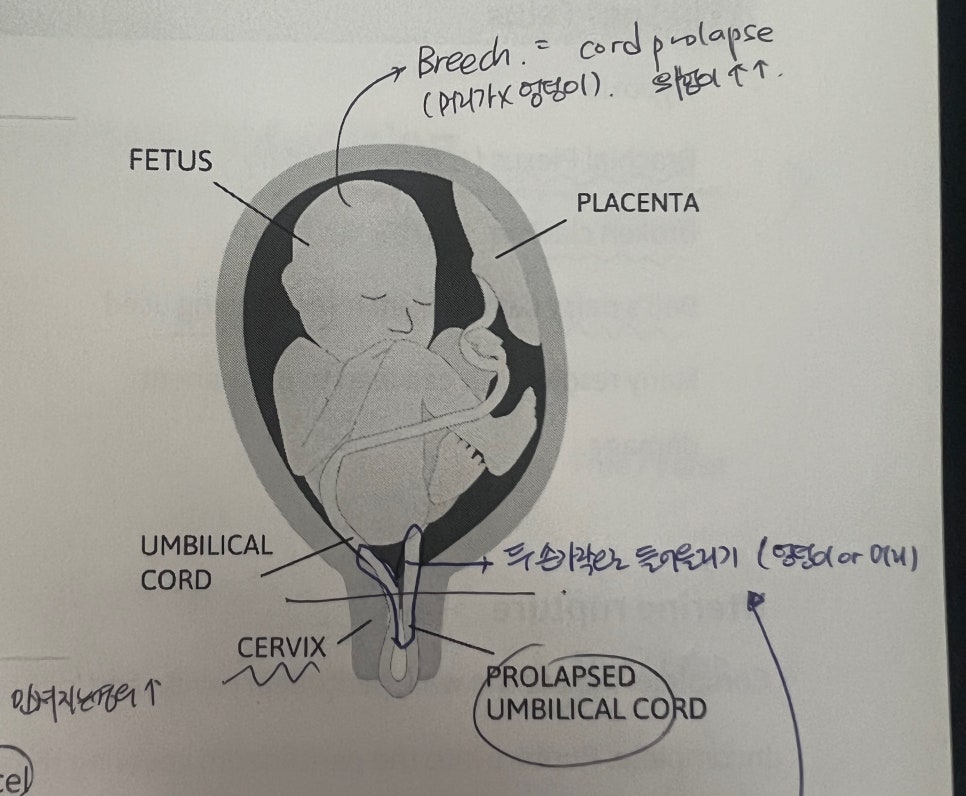
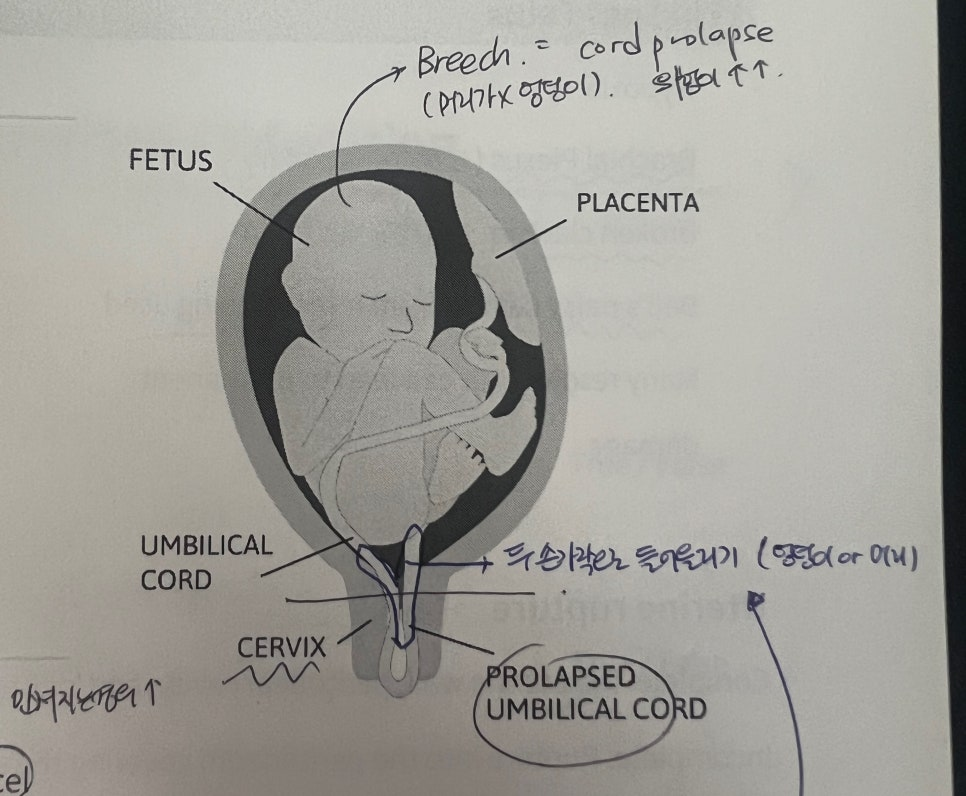
Prolapsed umbilical cord
1) Risk factors
-
Rupture of amniotic membranes
-
Abnormal fetal presentation
-
SGA : 공간이 넓어 빠져나올 위험이 커짐
-
Unusually long umbilical cord
-
Multifetal pregnancy : 다태아 임신
-
Polyhydramnios (양수과다증)
2) Findings
-
Visualization or palpation : 분만 중 내진 시 cord가 만져지는 경우가 많음
-
FHR monitoring shows variable or prolonged decel(2분 이상 지속됨)
-
Fetal movement; severe fetal hypoxia
3) Interventions
-
Do not leave the client
-
Call for assistance immediately
-
Insert two fingers and apply finger pressure on either side of the cord to the fetal presenting part to elevate it off
-
Knee-chest position or Trendelenburg
-
Assess FHR
-
Administer oxygen
-
Prepare for an immediate birth
Dystocia (난산)
: Difficult or abnormal labor related to the five P's of labor
1) Risk factors
-
Short stature, overweight status
-
Age greater than 40
-
Fetal head is larger than maternal pelvis : 태아 머리가 더 큼
-
Congenital anomalies : 선천적 이상
-
Fetal macrosomia (GDM)
-
Multifetal pregnancy : 다태아
2) Findings-Fetus
-
Hypoxia
-
Brachial Plexus (상신경종) injury : 쇄골신경 다칠 위험이 큼
-
Broken clavicle
-
Bell's palsy caused from forceps being used
-
Many resolve, but can lead to permanent damage
3) Findings-Maternal
-
Traumatic delivery leading to permanent damage.
-
Bruised bladder : 방광손상
-
Extension of episiotomy (회음절개술)
-
Rectal tear
-
Torn cervix and/or uterus
Uterine rupture (자궁파열)
Complete: the uterine wall, peritoneal cavity, and/or broad ligament, internal bleeding
Incomplete: Rupture into the peritoneum covering the uterus, but not into the peritoneal cavity, internal bleeding might not be present
1) Risk factors
-
Congenital uterine abnormality
-
Uterine trauma d/t accident or surgery(previous multiple c/sec births)
-
Tachysystole
-
Multigravida clients
-
VBAC
2) Findings
-
Sensation of "ripping," "tearing" or sharp pain
-
NRFHR
-
Change in uterine shape and fetal parts palpable
-
Hypovolemic shock: tachypnea, hypotension, pallor, and cool, clammy skin
3) Interventions
-
Administer IV fluids
-
Administer oxygen
-
Administer blood product transfusion if prescribed
-
Prepare the client for an immediate cesarean birth (possible hysterectomy)
-
Inform the client and their partner about the treatment
[ 헷갈린 부분 ]
-
Prolapsed cord는 탯줄이 만져지거나 보이는 경우로 손을 브이자 모양으로 만들어서 태아 머리나 엉덩이를 들어올리게 된다! c/sec 끝날때까지 들어올리고 있어야하는 것이 중요. 자궁 파열은 복부에서 fetal part가 만져지고 쇼크 증상을 보이는 것이 특징이며 똑같이 c/sec이 필요!
-
중력을 이용해서 cord 압박을 줄여야 하는것이라면 lateral position이 왜 안되는가?
옆으로 눕는 것은 중력 방향 변화가 거의 없음! 즉 태아가 위로 올라가지 않고 압박이 그대로 될 수 있기 때문에
Knee-chest position or Trendelenburg로 체위를 취해주어야함
[ 문제 ]
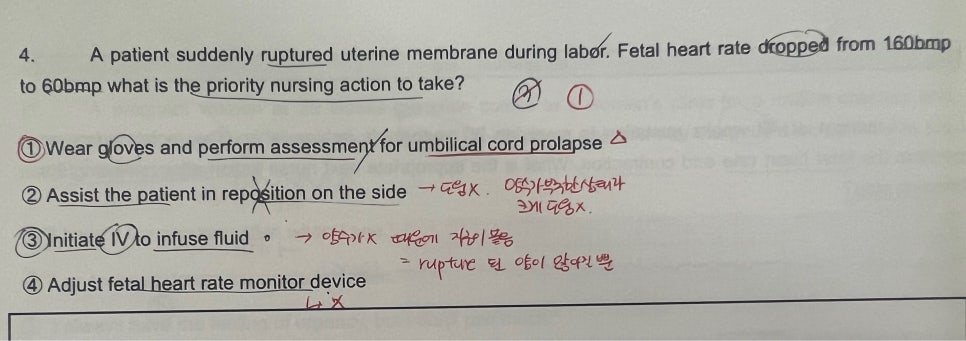
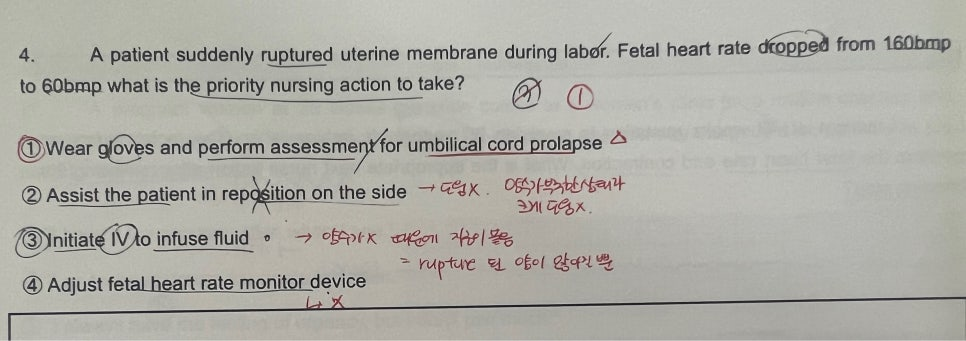
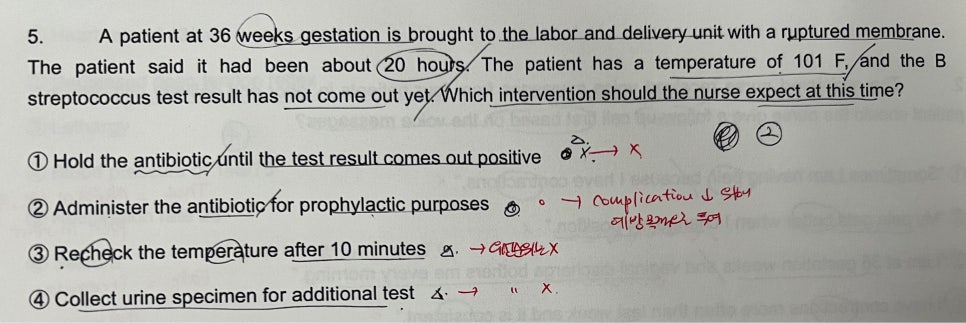
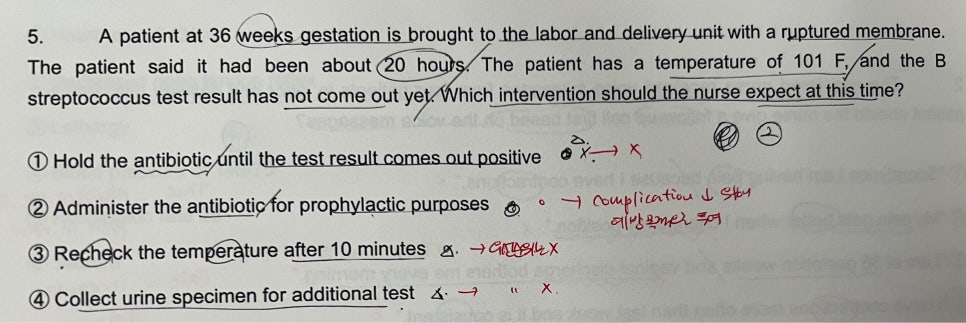
<내 풀이> 3번
1), 2) 양수가 없는 상황이기 때문에 크게 도움이 되지 않는다고 판단
3) 양수가 없는 상황이기 때문에 체액량를 보충해야한다고 생각해서 정답으로 고름
4) 할 수는 있지만 지금 당장 필요하지 않음
<정답> 1번
2) 양수가 부족한 상태이기 때문에 크게 도움되지 않음
3) 양수가 없는 상황이라 자궁이 붙어 있음, 수액 투여시 rupture 된 양이 많아져 더 위험
4) 할 수는 있으나 우선순위는 아님
[ 6주차 느낀점 ]
이번 주 학습을 통해 응급 상황에서 간호사의 신속한 판단과 중재가 얼마나 중요한지 느꼈다. 특히 제대탈출이나 자궁파열과 같은 상황은 짧은 시간 안에 태아와 산모의 상태가 급격히 악화될 수 있기 때문에, 이론을 정확히 이해하고 즉각적으로 적용하는 능력이 중요하겠구나.. 하는 생각이 들었다. 또한 실제 임상 상황을 떠올리며 반복적으로 복습하여, 위급한 상황에서도 당황하지 않고 정확하게 대응할 수 있도록 준비하고 다음 주차에도 열심히 학습해 보겠습니다!
[출처] https://blog.naver.com/kxnmin/224241546319

통신판매업신고번호 : 2024-서울서초-0152 | 출판사등록번호 : 제2019-000285호 | 개인정보관리책임자 : 김진선
주소 : 서울특별시 서초구 논현로31길 41, 5층(양재동, 세원빌딩) | 이메일주소 : dreamnurse7@naver.com
문의사항 : 드림널스 홈페이지 우측 하단 채널톡 문의 또는 카카오톡 채널 드림널스 문의 Copyright (c) 주식회사 드림널스 All Rights Reserved.
호스팅 제공자: 주식회사 맑은소프트