



 로그인을 해주세요
로그인을 해주세요
1. 심장의 기본 리듬
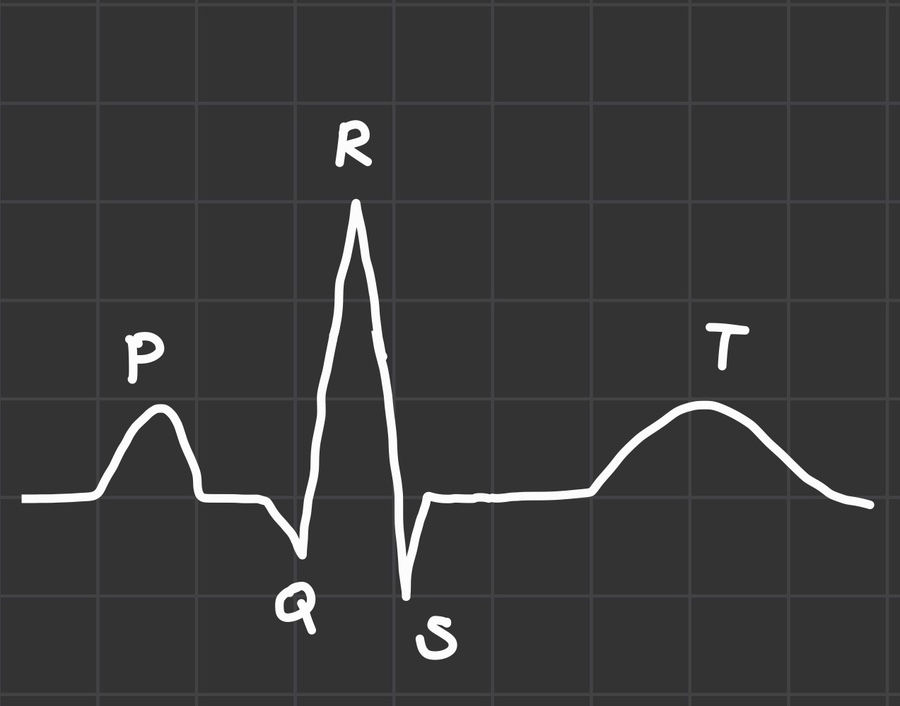
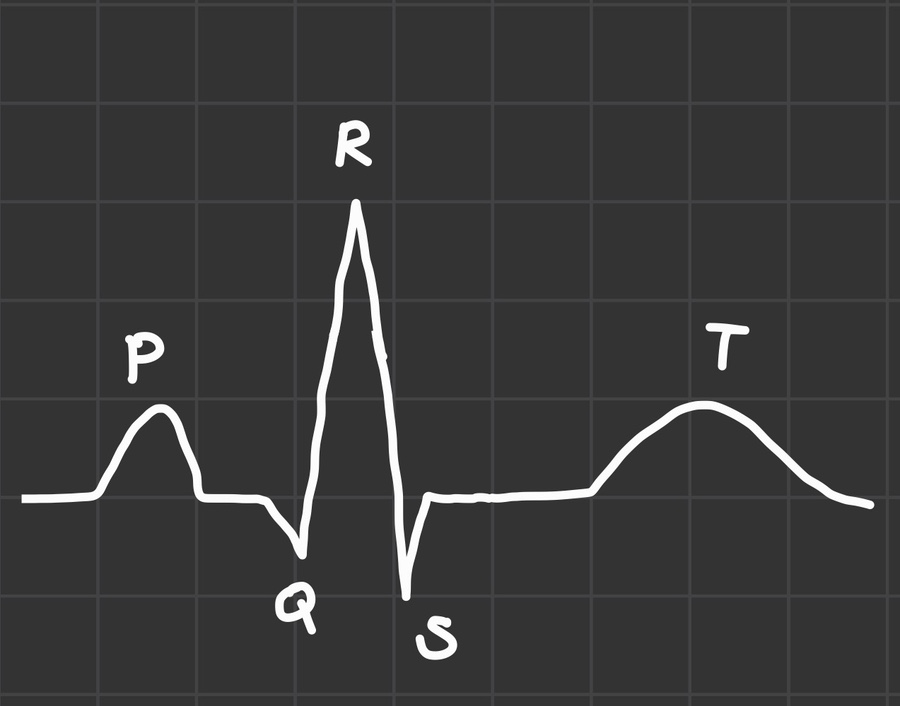
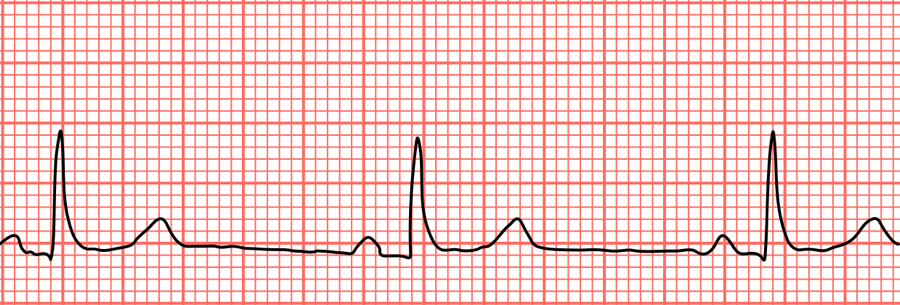
normal sinus rhythm
심방 수축 = P파
심실 혈액이 차는 시간 = PR interval
심실 수축 = QRS파
[특징] P-P, R-R 간격이 일정하며 규칙성을 가지고 있음. PR interval < 0.2sec
2. 부정맥 리듬
* 부정맥(arrhythmia) : 심장의 비정상적인 리듬
-> 정상 HR : 60-100회/분
-> 서맥(60회/분 미만), 빈맥(100회/분 이상) = 부정맥
Q) 정상적으로 심장이 뛰지 않았을 때, 무엇이 문제인가?
A) 심박출량이 줄어든다!
심박출량(cardiac output, CO) = 1회 박출량(stroke volume, SV) X 심박수(heart rate, HR). -> 서맥인 경우, 심박수가 느려지므로 심박출량이 줄어듦. -> 빈맥인 경우, 심박수가 빨라지나 충분히 혈액을 채우지 못하고 박출되기 때문에 1회 박출량이 줄어들어 심박출량 또한 줄어듦.
1) sinus arrhythmia
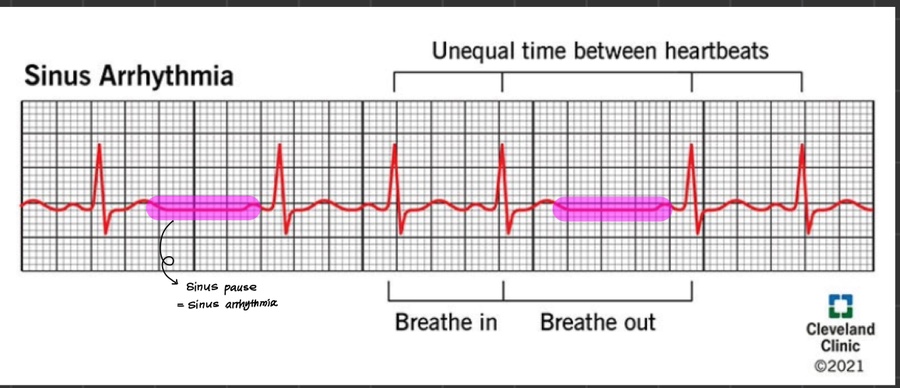
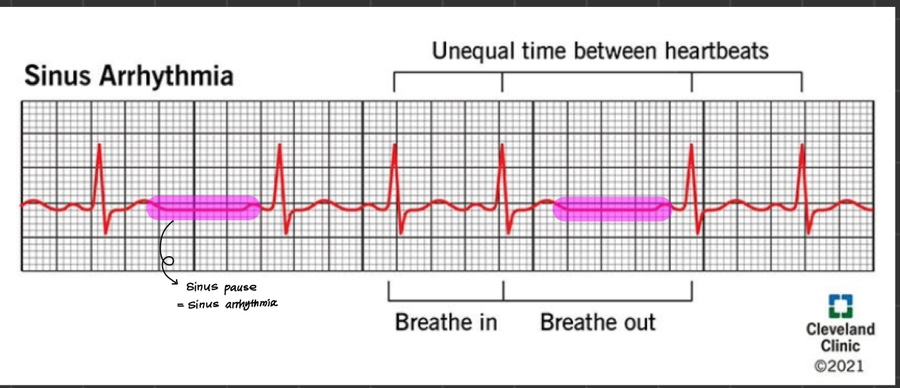
출처 : https://my.clevelandclinic.org/health/diseases/21666-sinus-arrhythmia
[특징] 모양이 일정하고 PR interval, QRS complex 모두 일정하나 R-R interval이 불규칙적
[원인] SA node의 불규칙(MI, 호흡기계 관련, digitalis toxicity, 부교감신경 항진)
-> sinus pause 구간이 너무 길어지거나 불규칙한 경우, 기절할 수 있고 이 때문에 pacemaker 넣는 경우도 있음
2. Sinus bradycardia & Sinus tachycardia
출처 : ACLS
[특징] PR interval, QRS complex, R-R interval 모두 규칙적이고 정상임
[차이점] 심박동수 속도 차이
-> 서맥 원인 : SA node가 느리게 페이싱(hypokalemia, hypothyroidism, beta blockers, calcium channel blockers, sedation, sleep)
-> 빈맥 원인 : SA node가 빠르게 페이싱(hyperthyrodism, bleeding, shock, exercise, stress, fever, dehydration, heart failure)
3. Sick sinus syndrome(=sinus nodal dysfunction)
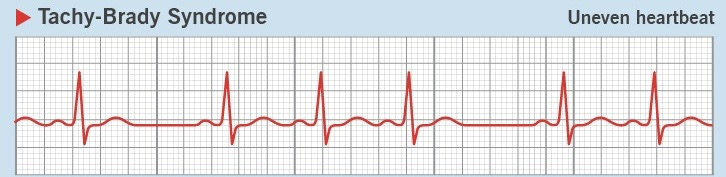
[특징] 불규칙한 심박동수(서맥이 있었다가 ~ 빈맥이 있었다가 ~)
-> 보상하기 위해 다른 pacemaker에서 뛰기 시작.
-> junctional rhythm이 나타나거나 PVC가 지나가는 경우도 있음.
[원인] SA node dysfunction(주로 MI로 인한 SA node 손상)
-> pacemaker 삽입 필요
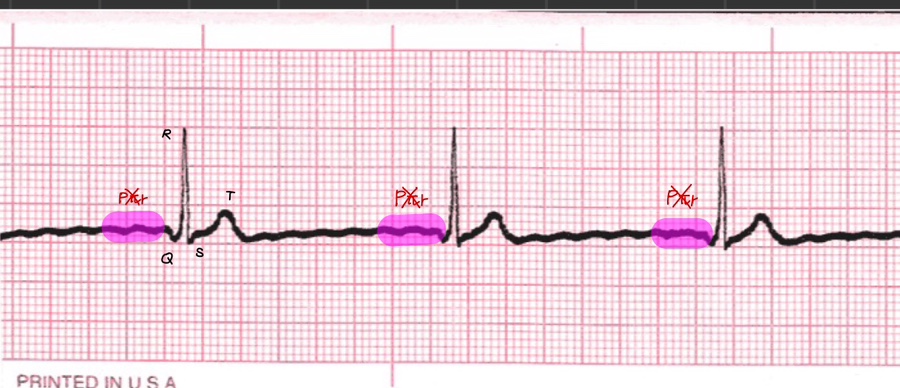
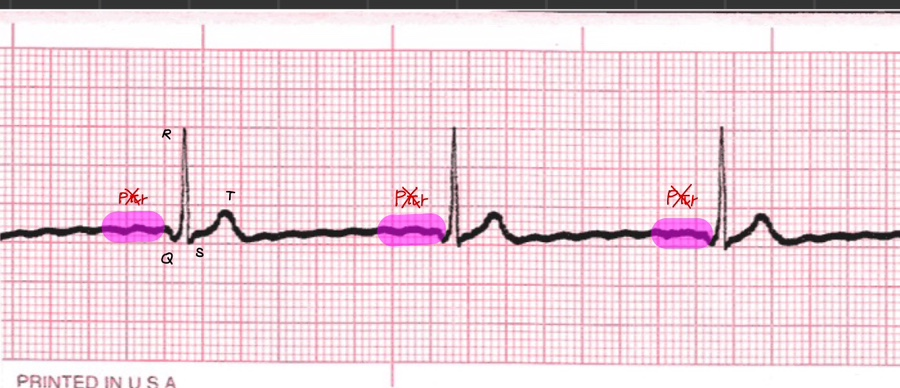
4. junctional rhythm
출처 : https://ekg.academy/lesson/37/junctional-rhythm
[특징] P파 존재하지 않음 = SA node dysfunction, HR 40-60회/분
-> AV node에서 시작
[원인] sick sinus syndrome, sinus dysfunction, severe sinus bradycardia, sinus arrest, sinus pause, AV block, hyperkalemia, antiarrhythmic medicaiton
- P파가 없으나 HR 60회 이상 = Acclerated junctional rhythm
- P파가 없으나 HR 100회 이상 = junctional tachycardia
5. Atrial flutter
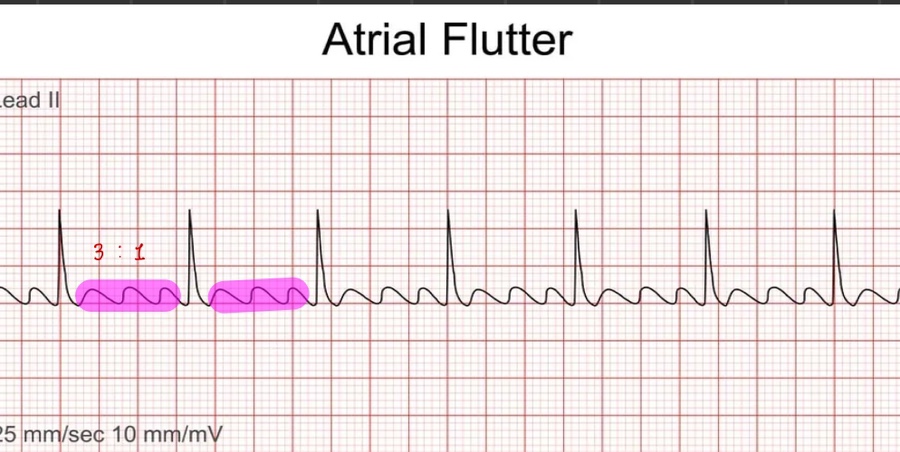
출처 : https://longmoreclinic.org/atrial-flutter-an-in-depth-exploration-of-a-heart-rhythm-disorder/
[특징] 톱니바퀴 모양 P파(=Sawtooth F wave), HR 240-360회/분
-> 전도 속도에 따라 R-R interval 규칙적이거나 불규칙해짐(2:1, 3:1, 4:1)
[원인] SA node보다 심방의 다른 부분에서 먼저 수축을 시작하면서 SA node의 활동이 억압됨.
6. Atrial fibrillation
[특징] 정상적인 P파 찾아볼 수 없음. HR 350-600회/분, R-R interval irregulary irregular
-> 심방 수축이 제대로 이뤄지지 않으므로 심실도 덜 채워짐 = preload 감소 = CO 감소
-> fibrillation이 색전을 유발하여 stroke 위험 증가
[원인] SA node보다 심방의 다른 부분에서 먼저 수축을 시작하면서 SA node의 활동이 억압됨.
[치료]
- if 환자가 stable, alert) HR controll
=> amiodaron bolus -> continuous iv infusion / beta-blocker
- if 환자가 unstable, recurrent) Rhythm controll
=> cardioversion
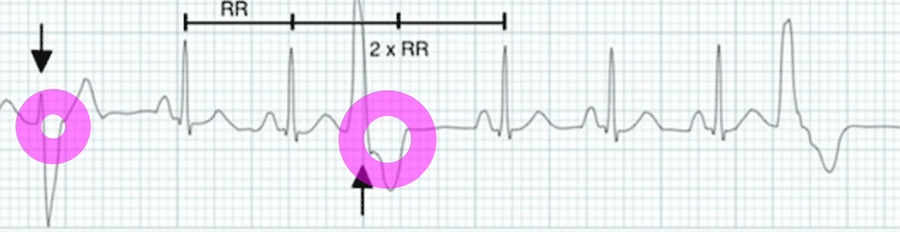
7. Premature atrial complex

출처 : https://my.clevelandclinic.org/health/diseases/21700-premature-atrial-contractions
[특징] P파는 정상이거나 매우 짧고 PAC point부분만 PR interval 및 R-R interval 불규칙적
[원인] Multiple sites in the atria or high in the AV junction
8. Premature ventricular complex(=PVC)
출처 : ACLS
[특징] wide QRS (>0.12sec)
[원인] ectopic site in ventricles(acute coronary syndrome, hypoxia, acidosis, hypokalemia, hypomagnesemia, heart failure, cardiomyopathy)
[치료] Replace electrolyte imbalance, hypoxia, acidosis, amiodarone or lidocaine
9. V-tach(ventricular tachycardia)
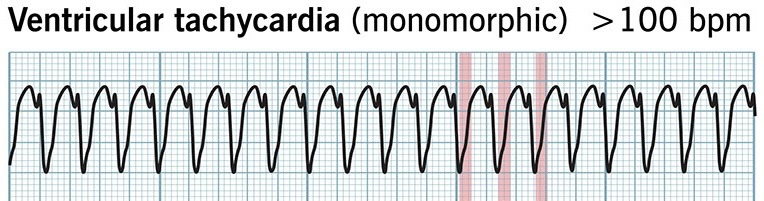
출처 : https://my.clevelandclinic.org/health/diseases/17616-ventricular-tachycardia
= PVC가 연달아 3개 이상 있을 시, v-tach으로 진행했다고 봄
[특징] P파 없음, wide QRS complex, R-R interval 규칙적, 맥박 유/무
Q) 왜 P파가 없을까?
A) 심방을 거치지 않으므로. 그렇기 때문에 심박출량(CO)도 감소한다.
if pulse가 있는 경우) 항부정맥제 IV + cardioversion !!
if pulse가 없는 경우 = pVT) priority : defibrillation!! -> compression
10. V-fib(Ventricular fibrillation)
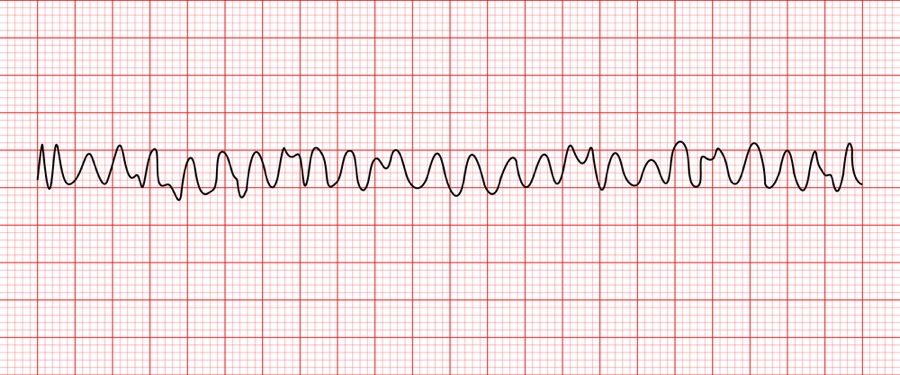
출처 : ACLS
[특징] 규칙성 X
priority : defibrillation!! -> compression
[문제]
A nurse went in to patient’s room and found out the patient is lethargic. Patient’s cardiac monitor was displayed as below. The nurse checked patient’s pulse and it was faint. Which is intervention is the priority?
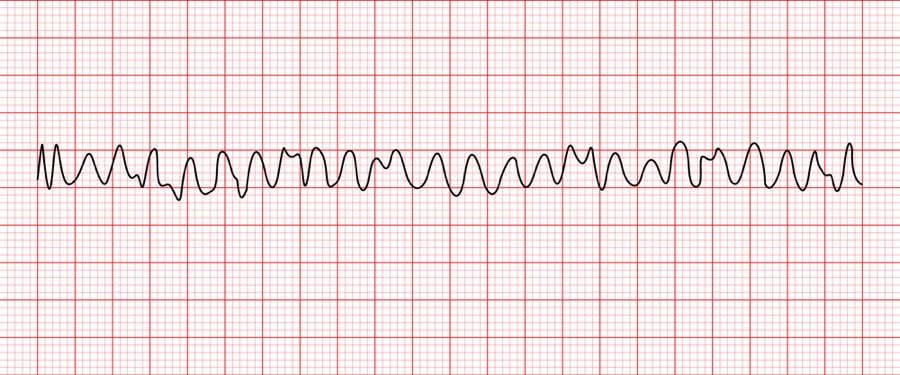
출처 : ACLS
1. Leave the room to bring the defibrillator.
2. Start chest compression and ask for help.
3. Give Epinephrine 1mg IVP.
4. Continue to monitor V/S.
=> 해당 사진은 V-fib으로 defibrillation이 우선이며 이후 cardiac compression, epinephrine IVP가 순차적으로 진행되어야 한다. 그러나, 보기 1번의 경우 제세동기를 가지러 가기 위해 방을 나가는 것으로 의식이 없는 환자의 곁을 떠나는 행위는 잘못 되었다. 그렇기 때문에 일단 심장 압박을 하며 동료들에게 제세동기를 가져달라고 도움을 요청하는 것이 정답이다.
11. Paroxysmal supraventricular tachycardia(=PSVT)
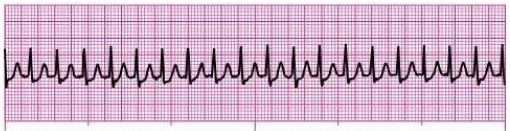
출처 : ACLS
[특징] HR 150-250회/분, 규칙성 있음
[원인] AV node에서 중복으로 수축
[치료] adenosine, cardioversion
8주차 공부 후, 느낀 점
: EKG는 정말 어렵다 ………… 그나마 드림널스 엔클렉스와 함께라서 이 정도까지 이해할 수 있었던 거지 혼자 공부하기엔 정말 막막한 파트임을 뼈저리게 느꼈다. 단순히 이론만 알려주는 게 아니라 리듬 파형을 보면서 공부하니 이해도가 높아졌고 중간중간 리듬 파형으로 퀴즈 내주시는 것도 먼저 심전도에 대해 생각해보기에 효과적인 공부법이었다. 아직도 완전히 내 걸로 만들진 못했지만 이번 기회에 꼭 마스터해야지!!!
[출처] https://blog.naver.com/luckyyy_402/224248295982


통신판매업신고번호 : 2024-서울서초-0152 | 출판사등록번호 : 제2019-000285호 | 개인정보관리책임자 : 김진선
주소 : 서울특별시 서초구 논현로31길 41, 5층(양재동, 세원빌딩) | 이메일주소 : dreamnurse7@naver.com
문의사항 : 드림널스 홈페이지 우측 하단 채널톡 문의 또는 카카오톡 채널 드림널스 문의 Copyright (c) 주식회사 드림널스 All Rights Reserved.
호스팅 제공자: 주식회사 맑은소프트