



 로그인을 해주세요
로그인을 해주세요
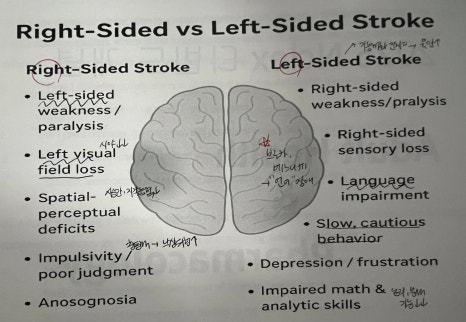
1. Right-Sided Stroke (→ Left Side deficits)
• Left-sided weakness/paralysis
• Left visual field loss / neglect
• Impulsive, poor judgment → HIGH fall risk
• Spatial-perceptual deficits
• Unaware of deficits (anosognosia)
2. Left-Sided Stroke (→ Right Side deficits)
• Right-sided weakness/paralysis
• Aphasia (Broca/Wernicke) → communication difficulty
• Slow, cautious behavior
• Difficulty with math, logic, analytical tasks
• Aware of deficits → anxiety, frustration common
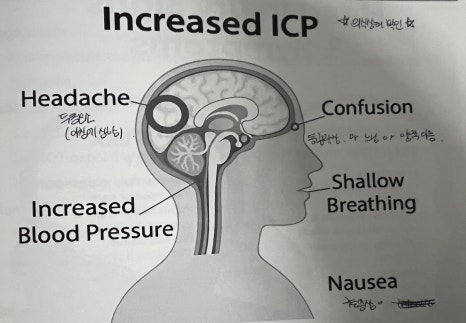
3. Increased ICP - Key Signs
• Decreased LOC (earliest sign)
• Headache (worse in the morning)
• Vomiting without nausea (projectile vomiting)
• Pupillary changes (unequal, sluggish, dilated)
• Cushing's triad:
• 1 SBP + Wide pulse pressure
• I HR (bradycardia)
• Irregular respirations
• Vision changes (blurred vision)
• Seizures
• Posturing (decorticate / decerebrate)
4. Head injury
1) Decreasing GCS
• Drop in GCS (especially < 8)
• Slower responses, confusion, can't follow commands
→ Earliest sign of worsening intracranial pressure
2) Unequal Pupils
• One pupil dilated, sluggish, or non-reactive
• Suggests brain herniation or compression of CN III
→ Medical emergency
3) Projectile Vomiting
• Vomiting without nausea
• Sudden, forceful → Indicates increased ICP
** Pattern Summary
GCS 1 + Unequal pupils + Projectile vomiting
→ Classic triad of worsening head injury / increased ICP
→ Requires immediate intervention and rapid neuro assessment
5. Enoxaparin (LMWH)
1) Mechanism
• Low-molecular-weight heparin that inhibits Factor Xa→ prevents clot formation.
2) Administration
• Given subcutaneously in the abdomen, at least 2 inches from the umbilicus.
• Do NOT expel the air bubble → helps deliver full dose and prevents bruising.
• No massaging, no aspiration.
3) Monitoring
• Platelet count is the key lab (risk of HIT).
• Hold medication if platelets < 100,000.-
• Routine PT/INR monitoring not needed.
4) Safety / Teaching
• Watch for signs of bleeding (bleeding gums, bruising, tarry stools, hematuria).
• Avoid NSAIDs and other anticoagulants unless prescribed.
• Use soft toothbrush and electric razor.
[ 헷갈린 부분 ]
1. Right-sided stroke와 Left-sided stroke의 행동 차이는 Right은 Impulsive (충동적), 위험 인지 못하게 되어 낙상 위험도가 올라가도 본인이 병을 앓고 있다는걸 모르게 됨!
Left는 반대로 Slow, cautious (느리고 신중함), 브로카와 베르니케 영역이 있으므로 Aphasia (언어 문제)가 발생하고 위와 반대로 병식 있기 때문에 불안, 좌절 증상이 나타남!
2. 항응고제니까 다 PT/INR 본다고 생각할 수 있지만 Enoxaparin (LMWH)은 Factor Xa 억제하고, PT/INR 모니터링 필요 없고, Platelet 확인만 필요!
Heparin은 당연히 aPTT 모니터링 필요! LMWH는 안 봄!
[ 문제 ]
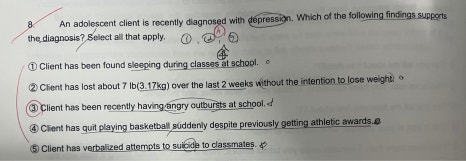
<내 풀이> 1, 2, 4, 5
-
저녁에는 불면이 있고 학교에서 잠을 자게 됨 -> 우울 증상o
-
뺄려고 하지 않고 체중 빠짐 -> o
-
크게 반항적이거나 화내는 모습은 보이지 않는다고 생각 -> x
-
운동을 열심히 하다가 그만둠 -> o
-
자살을 말로 표현 -> o
<정답> 1, 2, 3, 4, 5
-
불면이 나타나거나 잠이 많아 지게 됨 -> 정답
-
급격한 체중 변화 -> 정답
-
급발진, 반항적인 행동 또한 우울 증세의 일부 -> 정답
-
social withdraw로 볼 수 있음 -> 정답
-
자살 시도를 직접적으로 말로 표현 -> 정답
[ 9주차 느낀점 ]
이번 주에는 뇌졸중이랑 두부손상 내용을 공부하면서 생각보다 비슷한 부분이 많아서 헷갈리는 부분이 많았다. 특히 오른쪽, 왼쪽 뇌졸중은 단순히 마비 방향만 외우면 되는 게 아니라 환자의 행동이나 인지 상태까지 같이 이해해야 한다는 것이 새롭게 느껴졌다. 또한 ICP 상승에서 의식 수준이 가장 먼저 변한다는 점이 인상 깊었고, 이런 변화들을 빨리 알아차리는 게 정말 중요하겠다는 생각이 들었다. 약물에서는 Enoxaparin 투여 시 주의할 점이 생각보다 많아서 실제 임상에서 실수하지 않도록 더 익숙해져야겠다고 느꼈다!
[출처] https://blog.naver.com/kxnmin/224265791321


통신판매업신고번호 : 2024-서울서초-0152 | 출판사등록번호 : 제2019-000285호 | 개인정보관리책임자 : 김진선
주소 : 서울특별시 서초구 논현로31길 41, 5층(양재동, 세원빌딩) | 이메일주소 : dreamnurse7@naver.com
문의사항 : 드림널스 홈페이지 우측 하단 채널톡 문의 또는 카카오톡 채널 드림널스 문의 Copyright (c) 주식회사 드림널스 All Rights Reserved.
호스팅 제공자: 주식회사 맑은소프트