



 로그인을 해주세요
로그인을 해주세요
IM Injection Site for Infants
1. Most Appropriate IM Site for Infants
☛ Vastus Lateralis Muscle (Anterolateral thigh)
→ This is the preferred and safest site for infants (≤12 months)
2. Why Vastus Lateralis is Recommended
★ Anatomical Safety
• Few major nerves and vessels nearby
• Very low risk of nerve damage
★ Best Muscle Development
• Largest and most developed muscle at birth
• Provides consistent medication absorption
★ Easy Positioning and Stabilization
• Infant’s leg can be secured
• Staff and caregiver positioning is simple
3. Sites to Avoid in Infants (Common NCLEX Wrong Answers)
✗ Dorsogluteal (Buttock)
• High risk of sciatic nerve injury
• Insufficient muscle mass
• Poor absorption reliability
✗ Deltoid Muscle
• Underdeveloped during infancy
• Typically not used until ≥18 months–3 years
4. IM Injection Technique (NCLEX-Relevant Points)
✔ Angle: 90 degrees
✔ Stabilize the thigh during injection
✔ Landmark properly before inserting needle
✔ Z-track method may be used for irritating medication
Typical Needle Selection
• Gauge: 22–25G
• Length: ⅝–1 inch, depending on infant size
NCLEX-Style Application Example
“The nurse is preparing to administer an IM injection to a 3-month-old infant. Which site is most appropriate?”
✔ Correct answer → Vastus Lateralis (anterolateral thigh)
✗ Incorrect options → Deltoid, Dorsogluteal
Signs of Dehydration in Children
1. Key Physical Signs
• Dry mucous membranes
• Few or no tears when crying
• Decreased urine output (↓ wet diapers)
• Sunken eyes or sunken anterior fontanel (infants)
• Poor skin turgor
• Capillary refill > 2 seconds
2. Behavior & Vital Sign Changes
• Irritability or lethargy
• Tachycardia
• Weak peripheral pulses (advanced stage)
3. Urine Output Standards (Very Important)
• Infants: < 2 mL/kg/hr = concern
• Children: < 1 mL/kg/hr = concern
4. Most Common NCLEX Clues
• If you see these together → dehydration suspected:
✔ Dry mouth
✔ No tears
✔ Low urine output
Mononucleosis Precautions
1. Why Precautions Are Needed
Mononucleosis often causes:
• Splenomegaly
• Fatigue and sore throat
The main concern for NCLEX:
☛ Risk of splenic rupture
2. Activity Restrictions
Children/adolescents must:
⊘ Avoid contact sports
⊘ Avoid high-impact activities
⊘ Avoid abdominal straining
Examples:
Football, basketball, soccer, martial arts
Trampoline, heavy lifting
3. Duration
Typical recommendation:
☛ At least 3–4 weeks
But NCLEX emphasizes:
★ Wait until cleared by a healthcare provider (not just “feeling better”)
4. Warning Symptoms (Immediate evaluation)
Call provider or go to ER if:
⚠ Left upper abdominal pain
⚠ Left shoulder pain (referred pain)
⚠ Dizziness, fainting
⚠ Sudden weakness
→ These may indicate splenic rupture
5. Isolation
Standard precautions only
No special isolation needed
[ 헷갈린 부분 ]
1. 영아의 근 주사 부위에서 왜 dorsogluteal 부위는 사용하지 않는지 헷갈렸는데 처음에는 단순히 근육 크기 때문이라고 생각했다. 하지만 좌골신경 손상 위험과 약물 흡수의 불안정성도 중요한 이유라는 점을 다시 정리할 수 있었다.
2. 소아 탈수 기준에서 영아와 아동의 소변량 기준이 달라 헷갈렸다. 미세한 차이이지만 영아는 2 mL/kg/hr 미만, 아동은 1 mL/kg/hr 미만일 때 탈수를 의심한다는 점을 구분해서 외워야 한다는 것을 알게되었다!
[ 문제 ]
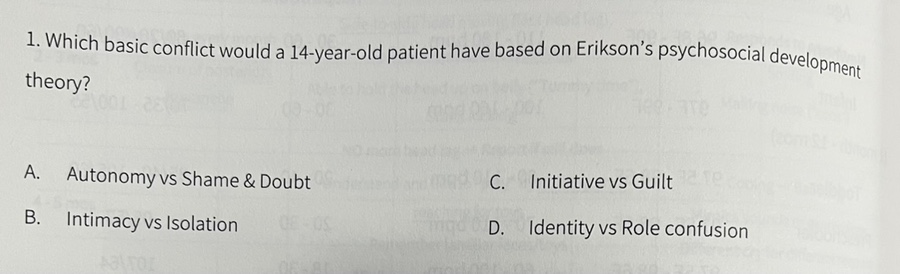
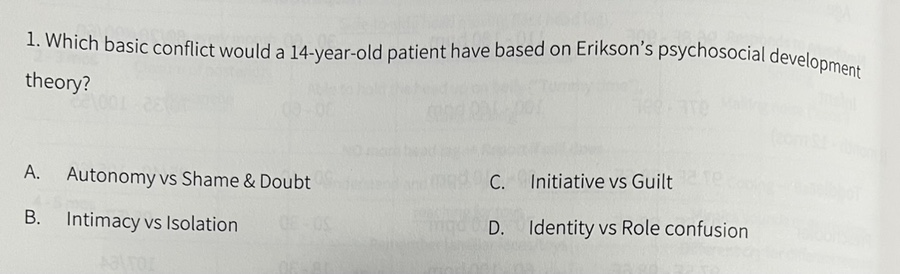
<내 풀이> D
A. 자율성~ 18개월에 시작
B. 친밀감 대 고립감 18세 이상에서 나타남
C. 주도성 대 죄책감은 3살부터 나타남
D. 정체성의 혼돈이 오는 시기는 12세부터이므로 -> 정답
<정답> 풀이 동일!
[ 12주차 느낀점 ]
이번 학습을 통해 소아 간호에서 자주 출제되는 핵심 내용을 정리할 수 있었다. 특히 영아 IM 주사 부위 선정 이유와 탈수 증상, 단핵구증 환자의 주의사항을 NCLEX 관점으로 이해할 수 있어 도움이 되었다. 단순 암기보다 왜 그런 간호를 적용하는지 근거를 함께 학습하니 기억에 더 오래 남았고, 실제 임상 상황에서도 적용할 수 있을 것 같다고 느꼈다 :)
[출처] https://blog.naver.com/kxnmin/224287993372


통신판매업신고번호 : 2024-서울서초-0152 | 출판사등록번호 : 제2019-000285호 | 개인정보관리책임자 : 김진선
주소 : 서울특별시 서초구 논현로31길 41, 5층(양재동, 세원빌딩) | 이메일주소 : dreamnurse7@naver.com
문의사항 : 드림널스 홈페이지 우측 하단 채널톡 문의 또는 카카오톡 채널 드림널스 문의 Copyright (c) 주식회사 드림널스 All Rights Reserved.
호스팅 제공자: 주식회사 맑은소프트